Introduction
With over 611.7 million hashtag views on TikTok,1 fasting and intermittent fasting is certainly well-known within the public sphere. But just how famous are fasting and its effects within the scientific and clinical realms? Aside from its popularity as a weight loss tactic, fasting has recently gained traction among researchers and clinicians as a potential natural intervention for IBD and other inflammatory conditions. Although the most touted dietary regimens have not always been found to be the most healthy, this emerging trend could flip the switch. Read on to learn about the five most common types of fasting, what the research says about the benefits and risks, and whether or not the evidence suggests any benefits of fasting for IBD.
What is fasting?
Broadly, fasting refers to a dietary restriction strategy involving reduced nutrient consumption for a specified time interval.2 Though an increasingly popular trend in the niche of “healthy lifestyles”, fasting is nothing new to humans and appears in several of the world’s oldest major religious traditions, including Ramadan, Yom Kippur, Lent, and Navaratri. While the historical motivations of fasting may include the spiritual, it turns out there are a number of potential health benefits as well to these periods of reduced eating.
Importantly, fasting (a dietary restriction-based strategy) isn’t inherently the same as caloric restriction (consuming fewer calories than you expend; typically 20-40% of normal caloric intake). While fasting may include an overall reduction in calorie consumption, caloric restriction is not the main priority of fasting; instead, fasting regimens—like intermitted fasting (IF) and periodic fasting (PF)—can focus on reduced intake of a specific dietary component (generally macronutrients like protein, fat, or carbohydrates) or specific periods of time for reduced nutrient intake.
Caloric restriction on its own has been demonstrated to improve some age-related changes and immune processes3–5 as well as reduce the risk of several conditions like diabetes, cancer, and cardiovascular disease.3,6,7 However, when caloric restriction is implemented on a constantly recurring and/or persistent basis, all those missing calories can start to add up to extremely low body mass index (BMI)3,6,7 or diminished immune function.3,8,9 The body needs fuel to work! Therefore, periods of fasting can confer some of the benefits of reduced nutrient intake while mitigating some of the harmful side effects of overapplying caloric restriction.
The proper functioning of the brain and other active tissues (such as blood cells) is fueled entirely by glucose (sugar), so glucose must always be readily available in the bloodstream for a person to survive. Accordingly, glucose levels primarily determine the body’s nutrient state. Fasting decreases blood glucose levels in the blood, which thereby alters the nutrient state of the body. This in turn modifies the release of metabolic hormones from the liver to normalize blood glucose levels, such as glucagon (increases blood glucose levels) and insulin (decreases blood glucose levels). In summary, the nutrient state dictates hormone release from the liver to provide the brain and other active tissues with the fuel they need in states of altered nutrient intake.3,10,11 Thus, fasting derives its benefits from metabolic changes to the nutrient state (aka glucose levels) and is ultimately driven by the brain’s and other active tissues’ energy needs.
Common Types of Fasting
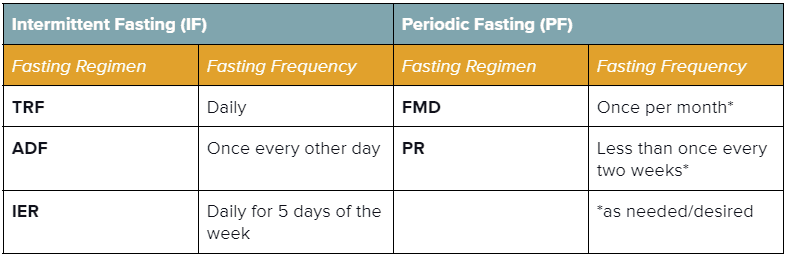
There is a huge range of what people mean when they use the term “fasting”, and in truth, there is no one “right” way to go about it! Dietary strategies of any kind are deeply individual to a person’s metabolic needs and access to different foods. Fasting strategies generally fall into two categories: Intermittent Fasting (IF; shorter repeating intervals of fasting and eating) and Periodic Fasting (PF; longer intervals of fasting paired with unrestricted eating intervals; can be either repeated or done as needed).3 Below is a breakdown of the five most common types of fasting3,12 to help you and your healthcare team determine if, and which type of, fasting might be appropriate for you to explore. It is important to note that although there have certainly been some promising evidence presented supporting the benefits of fasting, this research remains in its infancy and should only be started following approval by and under the supervision of your healthcare professionals (more on this later).
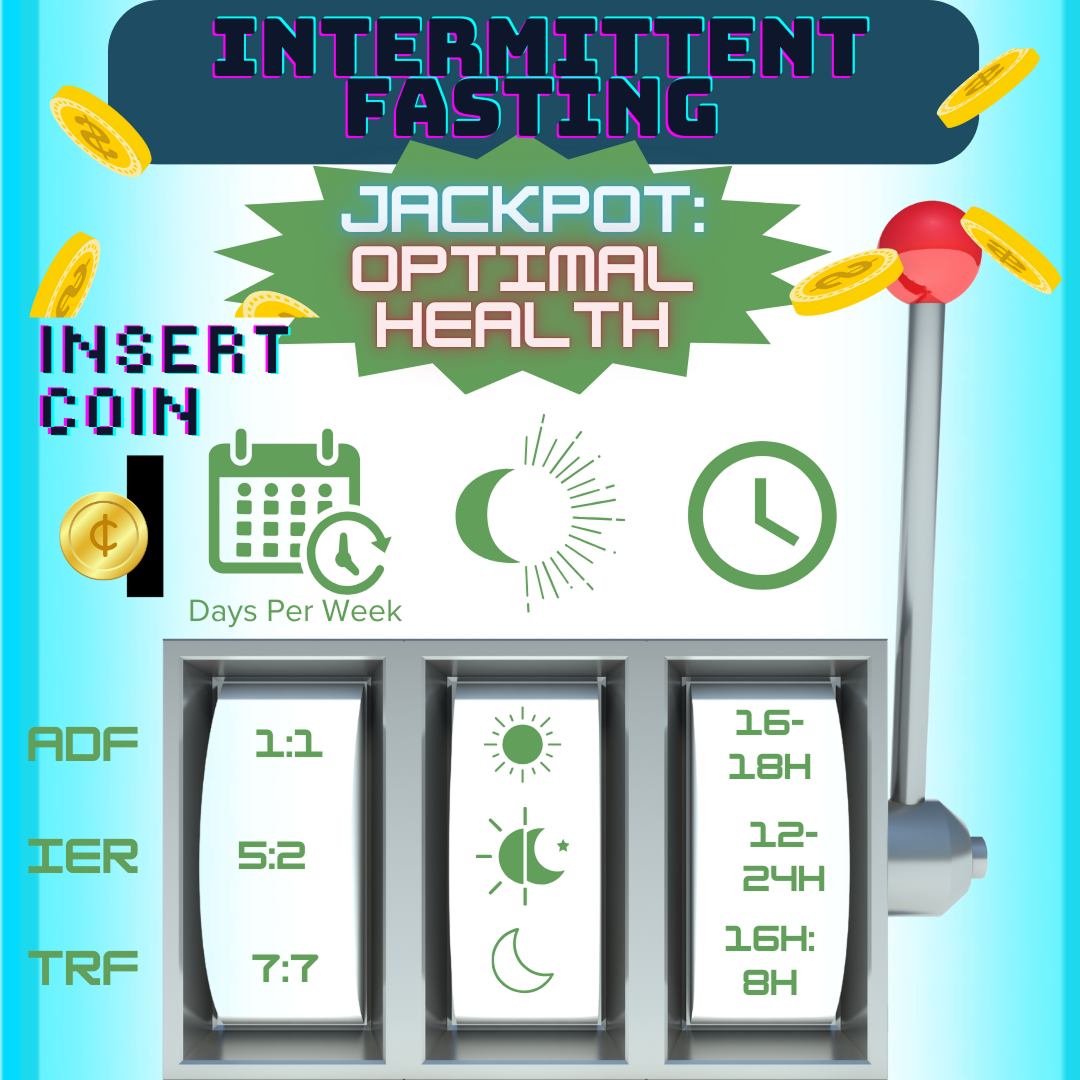
| Intermittent Fasting (IF)3,12 Alternating between intervals of short fasting or reduced nutrient intake (16-48 hours) and eating (8-120 hours).3,12 | Periodic Fasting (PF)3Either entirely restricting (‘water-only) or drastically reducing caloric intake (‘FMD’) for a prolonged time (>2 days; ~2-7 days); accompanied by an ad-libitum (unrestricted) refeeding interval3 |
|---|---|
| Time-Restricted Feeding / Fasting (TRF)Designating a restricted time interval (typically ≤12 hours) each day for eating. Sometimes referred to as ratios (e.g., a 16:8 fast is 16 hours of fasting & 8 hours of eating per day). This type of fasting is common in religious practices like Ramadan and Tzom Gedalia.3 | Fasting-Mimicking Diet (FMD)A monthly interval of reduced (30-50% of normal) caloric intake for ~4-7 successive days, accompanied by an ad-libitum (unrestricted) refeeding interval (generally 10-25 days). This type of fasting is typically employed as a plant-based diet comprised of foods with low protein, low carbohydrate, and high unsaturated fat.3 |
| Alternate-Day Feeding / Fasting (ADF)Alternating between intervals of short fasting or reduced nutrient intake (16-48 hours) and eating (8-120 hours).3 | Prolonged Fasting (PR)An extremely calorie-restricted or water-only fasting interval (~2-7 days, sometimes up to 21 days), accompanied by an ad-libitum refeeding interval of 7+ days; may be done periodically or as needed (no more than once every two weeks).3 |
| Intermittent Energy Restriction (IER) Limiting energy intake (20-25% of daily energy needs) on designated fasting days (i.e., 5:2 diet, 5 non-fasting days & 2 fasting days).12 | NOTE: Periodic Fasting must be carried out under specialized medical supervision to prevent detrimental effects on health. |
Both intermittent fasting (IF) and periodic fasting (PF) have gained recent attention from the health and science communities due to their newly discovered potential benefits in improving longevity and healthspan.2,3 As a result, IF and PF have been proposed as promising therapeutic avenues for several inflammatory conditions, including IBD, psoriasis, and rheumatoid arthritis (RA).2,3,13
Proposed Benefits of Fasting
Because the essential idea of fasting—intervals of less nutrient intake and more nutrient intake—comes in varied flavors, each of the above strategies can elicit a range of physiological effects, and so the respective benefits and risks warrant individual consideration. In addition, fasting operates within the context of your own unique biology, so results can vary between individuals. Fasting is not a monolithic dietary intervention, and each study has taken a slightly different angle. These research variations—especially when combined with the current sparsity of data on individuals outside of what is considered the “general population”—can make results a challenge to compare and limits the research’s application in understudied populations. That being said, there are a few proposed benefits and risk considerations that are worth mentioning!
As you can see, regulation of nutrient intake through periods of fasting can have wide-ranging effects across general human health in some of the trickiest conditions, especially in those that develop slowly over time as disruptions to normal immune function (such as in inflammatory conditions, cancer, and neurodegeneration). Can the numerous physiological benefits of intermittent fasting translate to meaningful benefits for people living with inflammatory bowel disease?
Fasting and IBD
While fasting has been associated with numerous benefits across a wide range of health concerns, four of the areas discussed above that are most relevant to IBDers include:
- Reducing inflammation.
- Reversing gut dysbiosis.
- Enhancing epithelial barrier integrity.
- Improving stress resistance and protection against chronic diseases like cancer.
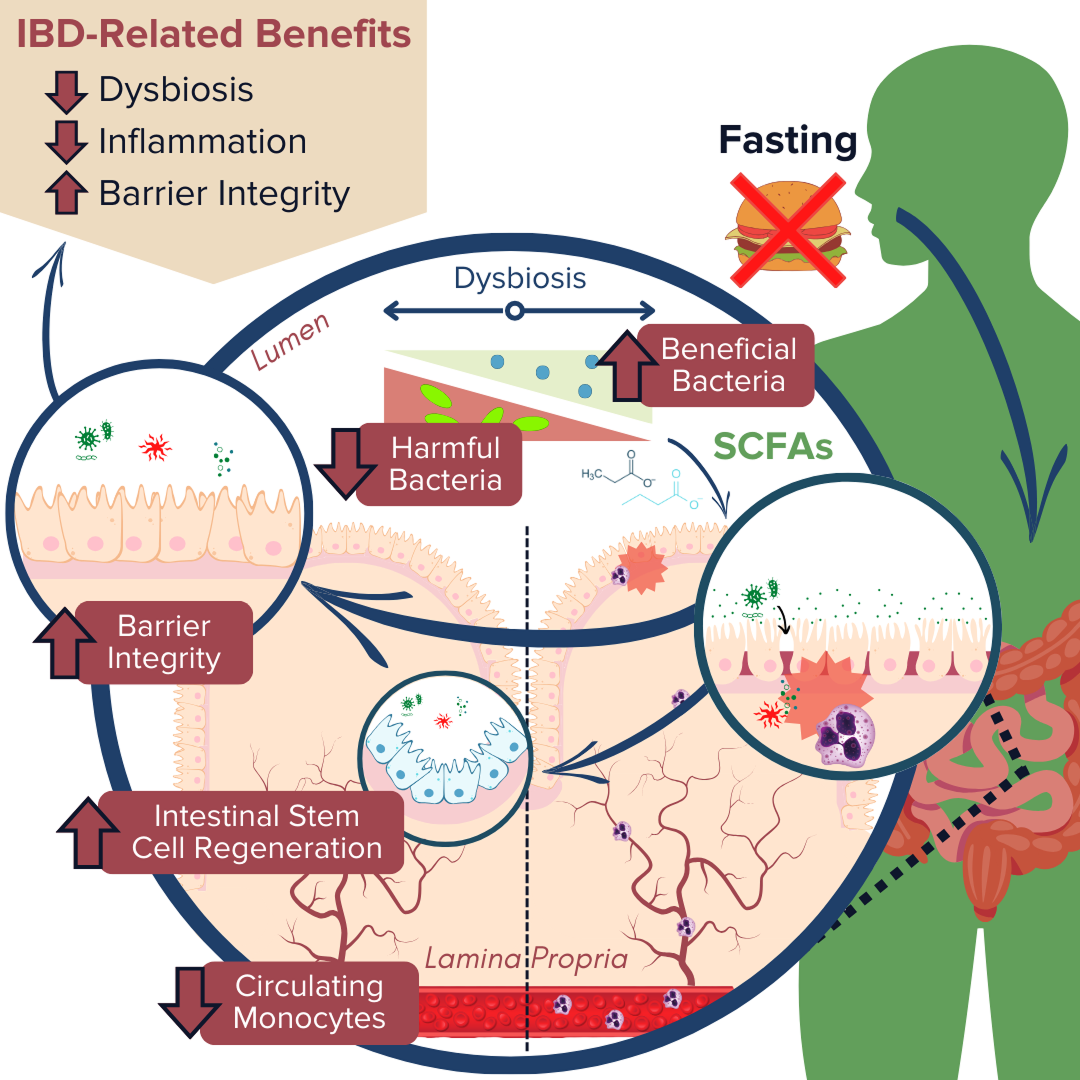
IBD pathogenesis is characterized by dysbiosis of the gut microbiome and increased intestinal permeability, which fuel a runaway inflammatory response that can further exacerbate dysbiosis and damage to the intestinal barrier.78–81 Fasting poses a unique opportunity for disrupting this positive feedback loop based on the proposed benefits of improving gut microbiota composition, enhancing epithelial barrier integrity, and reducing inflammation.13,20–22,82,83 Together, tackling these three mechanisms of inflammatory bowel disease demonstrates that fasting may be a promising avenue to support healing and IBD symptom relief.
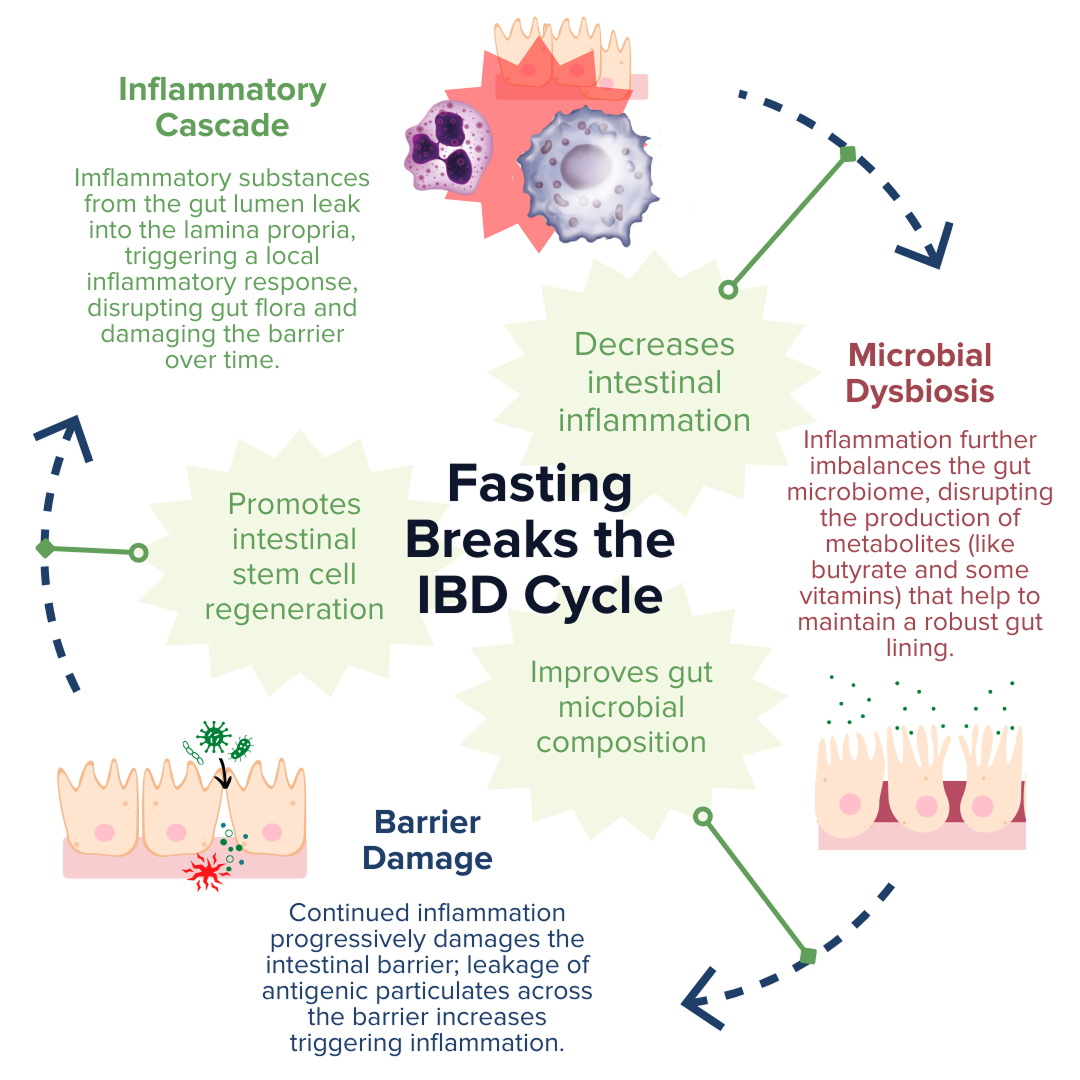
Production of SCFAs (such as butyrate, propionate, and acetate) by beneficial gut microbes (such as A. muciniphila) is involved in maintaining proper gut barrier function and regulation of intestinal inflammatory responses.13,20,21,84 For example, fasting has been shown to positively alter microbial diversity within the gut to promote the production of bacterial-derived SCFAs (such as propionate).20,21 These SCFAs can encourage the regeneration of intestinal cells and nourish the epithelial barrier, thereby enhancing gut barrier integrity, reducing leakage of antigenic (immune response-triggering) particulates from the gut lumen, and subsequently alleviating inflammation and preventing further damage to the barrier by immune cells.20,21,67,84 Another notable study recently reported that employing FMD cycles in a mouse model of colitis was able to ameliorate IBD-related pathologies by improving the microbial composition within the gut, decreasing intestinal inflammation, and promoting intestinal stem cell regeneration.13
Ultimately, numerous animal studies have supported these beneficial effects of fasting on the three molecular mechanisms associated with IBD pathology. Human studies have also supported these findings. However, few of these studies have assessed these effects in individuals with clinically-diagnosed IBD, and so more research is needed to understand the direct impact of fasting on treatments and symptoms of ulcerative colitis and Crohn’s disease.2,3,11,12,83
Risks of Fasting
While fasting comes with a range of possible benefits for general health and IBD alike, as with any intervention, it is not without risk. Fasting causes a disruption, by design, to the nutrient state of the body. Because nutrient absorption is already a known issue in people with Crohn’s disease and ulcerative colitis, additional restriction of food intake can exacerbate malnutrition and lead to additional downstream effects on mood and stress. Specifically, poorly planned fasting regimens can lead to:
In addition to the considerations noted above, a recent review70 published to guide physicians on fasting recommendations proposed that individuals who are under 18 and over 75, have a history of disordered eating, qualify as underweight status for Body Mass Index (BMI), are pregnant and/or breastfeeding, and/or have Diabetes Mellitus (type 2 diabetes) refrain from fasting. Thus, potentially more severe adverse effects may be possible in these populations.
Given these risks, it is all the more critical for people to be under the supervision of a healthcare professional to identify a fasting strategy tailored to their unique biology to monitor for and mitigate negative effects.
Notable Limitations of the Current Research
While fasting is being discussed more and more for a wide range of benefits, the available research is still in its infancy and (like with all research) has its limitations. As has been duly noted by multiple reviews on the effects of fasting on human health2,3,11,12,83,108, there are some notable gaps in the experimental evidence that warrant clarification and should thus be taken into consideration if fasting is something you might like to try.
Although the effects of fasting have been intensively studied for years, human studies have been predominantly restricted to healthy adult populations.2,3,11,12,83,108 Recent research on the effects of fasting on Crohn’s disease and ulcerative colitis have thus far been limited to mostly in vivo animal models of experimental colitis and in vitro tissue culture studies, so their application to humans is inherently limited. The few human studies that have been performed to date have not only yielded mixed results, but also were investigated in small groups of study participants, were conducted for a relatively short duration, and have provided very limited evidence on the impact of fasting in patients with CD.2,3,11,12,83,85,86,108 A clinical trial (NCT04271748) that launched in 2021 is currently investigating the effect of TRF on the gut microbiome and clinical outcomes in patients with Crohn’s.109,110 Even so, the IBD Centre of British Columbia has concluded that there is not yet enough evidence to advocate the therapeutic use of fasting for IBDers.85
The Fasting Trifecta
We’ve discussed the various types of fasting and some potential benefits and risks, but how exactly might one incorporate fasting into their life? There are three critical variables to consider before and throughout your fasting experience: type and frequency of fasting (how and how often you fast), time window of fasting (when you fast), and duration of fasting (how long you fast for).
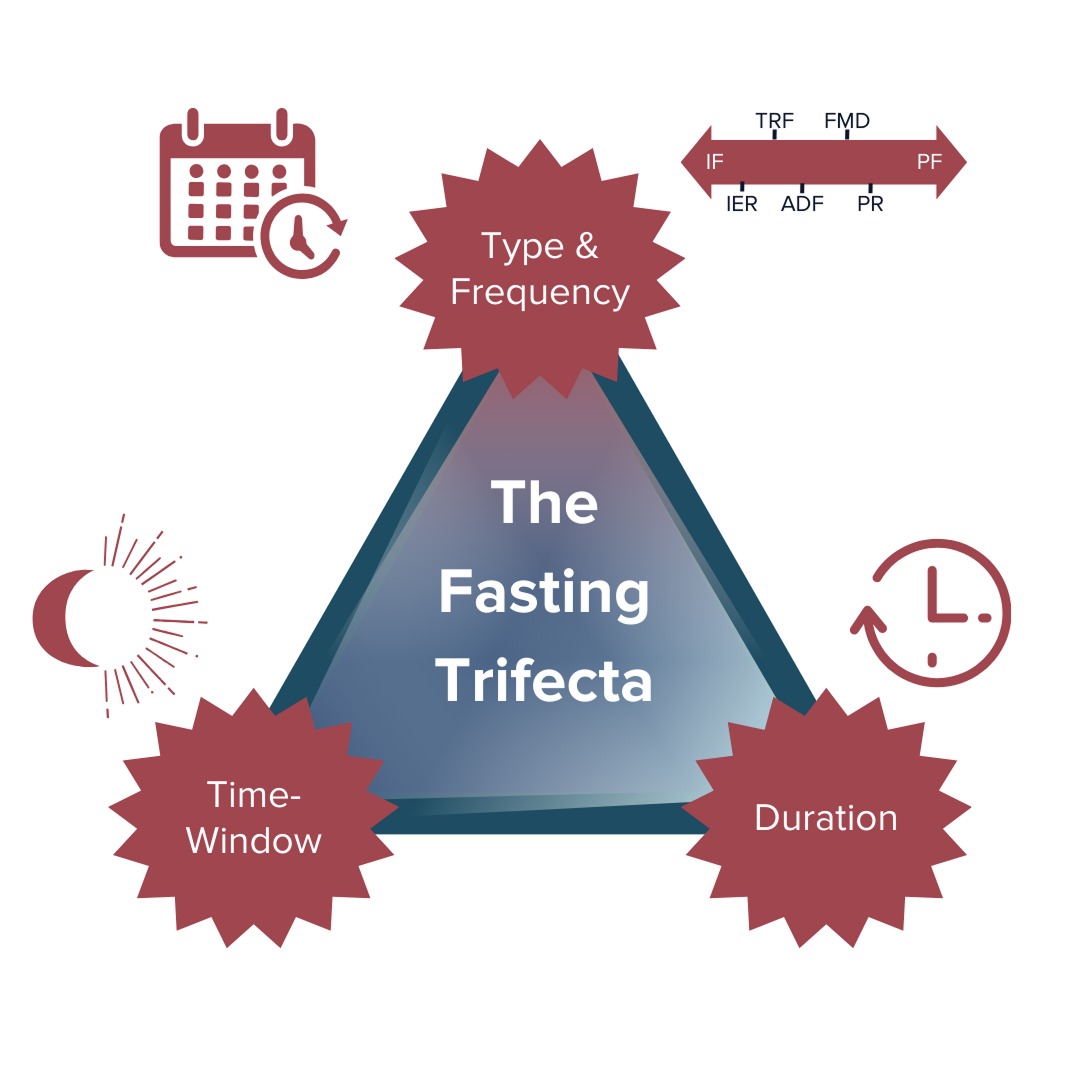
How well a fasting regimen (if any) will work for each individual depends on the type of fasting and the ‘fasting trifecta’ variations and combinations we choose (or don’t choose) to pursue. Our specific biologies, environments, lifestyles, other behavioral characteristics, and countless other factors all come together to determine the best combination of the trifecta that may work the best for each of us individually.
Fasting Type & Frequency (How and how often you choose to fast)
How You Choose To Fast: There are a variety of fasting regimens to choose from, starting with the decision between IF or PF. PF (especially prolonged fasting) is not generally recommended for individuals with CD due to the high risk of malnourishment and related complications.2,3,12,85–88 Although specific variations of PF (like FMD) may have some benefit for the IBD community, there is not enough evidence yet to conclusively advocate its therapeutic use for IBD.85
From there, you can choose which variation of the two (i.e., TRF, ADF, or IER; and FMD or PR) will work best for you! You can use the table from the above section (‘Common Types of Fasting’) as a starting point to explore which ‘how’ might be able to meet your needs.
How Often You Choose To Fast: Frequency of fasting refers to the number of times the fasting regimen is repeated within a designated interval or fasting cycle. Interestingly, the refeeding period associated with fasting appears to enhance its regenerative capacity compared to strict CR.3,75(p1),111–113 For each of the five mentioned fasting regimens, examples of their frequencies include:
Fasting Time-Window (When you choose to fast)
Research has shown that time of day heavily influences the impact of fasting. Studies suggest fasting during the evening rather than the day may sync metabolic patterns with circadian biology by aligning food intake with optimal metabolic hormone responses.12
Fasting Duration (How long you choose to fast for)
The type of fasting regimen pursued (i.e., IF vs. PF) will primarily determine the duration of fasting. Duration of fasting refers to the length of time spent in fasting periods (rather than non-fasting) within a given fasting cycle. A recent review3 highlighted the critical role that much shorter (rather than continuous) fasting intervals play in mitigating the adverse side effects associated with chronic DR strategies. Evidence suggests that approximately 12-hour fasting or TRF intervals may offer the most beneficial health effects due to the apparent absence of known harmful effects.3
However, certain fasting intervals can work better or worse for your specific biology within the variations of each regimen (i.e., TRF, ADF, and IER; PR, and FMD).
Examples of Trifecta Combinations from the Scientific Research:
IF for 12-48 hours done every 1-7 days and PF for 2-7 days done once or less per month may harness the capacity to ward off and improve disease activity;3 however, research definitively identifying its impact on cellular aging processes, the mechanisms at play, and how these mechanisms interact with the primary mechanisms active in IBD pathology is still in its infancy.3 PF can be repeated but should not be done frequently (less than once every two weeks, >1x/2 weeks).3
Personalizing Your Combination of the Fasting Trifecta to ‘Hit the Jackpot’
Now that we’ve reviewed some common fasting types and potential benefits and risks, you can use this information to help determine which combination of the fasting trifecta might work best for you!
To help us understand the relationship between each of these variables within the context of fasting, let’s consider the simple analogy of winning on a slot machine:
Generally, we can think of fasting as the slot machine, with each variable as its own wheel on the machine. The goal of the slot machine is to hit the jackpot; with fasting, we can broadly define the ‘goal’ as achieving optimal health benefits for an individual’s unique biology. All three wheels must align just right to hit the jackpot with the best combination of fasting frequency, window, and duration!
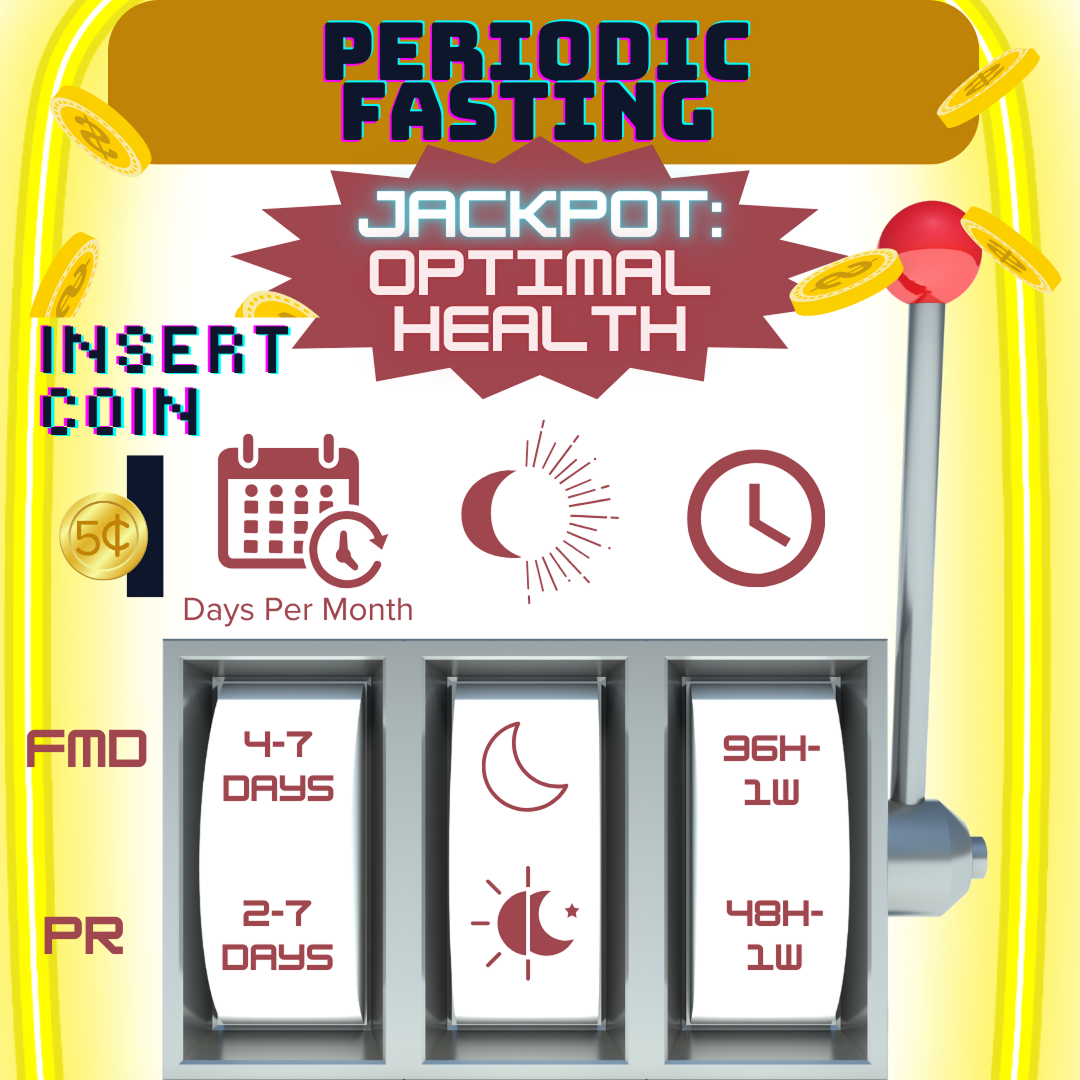
Hitting the ‘Jackpot’ of Fasting Outcomes: Different combinations of the fasting trifecta’s variables will work differently for each person’s biology. The first choice is deciding which ‘slot machine’ to play (the equivalent of choosing which type of fasting to explore). Then we can ‘play to win’ by pulling the lever, which generates a fasting trifecta combination (the equivalent of exploring one combination of the fasting trifecta’s variables). Whether or not this combination is your ‘jackpot’ will be partly determined by which fasting category and associated regimen you chose to pursue, but also by your own unique contributing factors (such as your biology and lifestyle).
Key Takeaways
Research suggests that significant fasting benefits could include improved overall metabolic health, longevity, and healthspan. However, the use of fasting regimens—particularly the more prolonged and severe variations—also carry unique risks for IBDers (especially those with Crohn’s disease), including weight loss, malnourishment, and worsening of current micronutrient deficiencies. Although some promising research has been accrued to support the benefits of fasting in healthy adult individuals, there is still not enough evidence in humans to definitively advocate its therapeutic use for IBDers. How well a fasting regimen (if any) will work for any one person depends on not only the particular combination of the “fasting trifecta’s” variables, but also on how that combination interacts with their specific biology, environment, lifestyle, other behavioral characteristics, comorbid conditions, and countless other factors. This can make the pursuit of fasting feel overwhelming, but ultimately it means there is room for choice and customization.
All forms of fasting should only be pursued after consulting with and notifying your healthcare team. If you and your healthcare team think that fasting is something you’d like to explore, consider how the “fasting trifecta’s” variables—type and frequency of fasting, fasting time window, and fasting duration—might work best for your medical and lifestyle needs.
Are you interested in learning how to leverage your own unique biology to craft a rounded IBD remission protocol that’s tailored specifically to meet your unique needs and goals? IBDCoach has developed a comprehensive Remission Master Plan to help empower IBDers to use their knowledge to fight back against IBD. Enroll in our Free Online Microcourse: The Foundations of Remission, or Schedule an Admissions Call to learn how to get started today!